
In this section, Dr. Sastry describes two of the changes she has made to the course since it was first offered, as well as the motivations behind those changes.
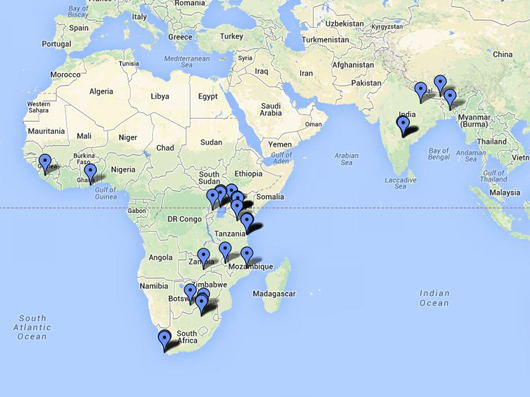
Project sites for GlobalHealth Lab from 2008–2013. Map data ©2013 Google. All rights reserved. This content is excluded from our Creative Commons license. For more information, see http://ocw.mit.edu/help/faq-fair-use/
Broader Geographical Scope
In our first few sets of projects, we only looked at sub-Saharan Africa. At one point, we were learning about setting up a contract or fee-based clinical lab service in Zambia. The students were trying to benchmark by visiting lab companies here like Quest Diagnostics. I quickly saw that while it is great to do work in our own backyard and look at local examples, it clearly is not the only benchmark. It made sense to ask, who else was doing high-volume, high-efficiency, low-cost medical services? Since we were seeing similar things in South Asia, I realized that we should be looking at other settings too, and it seemed natural to pair South Asia with sub-Saharan Africa because of their similarities and some of their differences.
There are some fascinating opportunities and learning that can cross borders. Sub-Saharan Africa, especially East Africa and some parts of South Africa, have some amazing innovations using cell phones, SMSing, micropayments, and other methods. Social capital, technology, and social structures are leveraged in ways that are not as visible in South Asia. South Asia has not innovated as much in the mobile space, but they have great methods for community and village-based care. We see amazingly efficient hospitals in India and wonder how they can translate to other settings. So we have broadened our scope to include South Asia, namely India, Bangladesh, and Nepal.
More Rigorous Selection of Hosts
When this course was first offered, we were willing to work with anyone. We then learned that when working with for-profit companies trying to reach the very poor, we had to really invest in understanding whether the project would pan out because almost all of them did not. This leads to some really interesting research questions. Why is it so hard to serve the poorest of the poor? Many people think that if you are good at serving the middle class and have figured out how to scale up, you should be able to adapt that to serve the very poor. It’s not that simple. Now we have a screening question that says, “Do you currently serve the poor?” If an organization currently does not, maybe we should not work with that organization if our current goal is to serve the unreached populations. So, I have learned to think carefully about our partners if we want to uphold such a specific focus.
We always want to be really focused on point of care and to have students interact in a setting where patients or community members are receiving care. But I get constant pressure to move to different parts of the value chain. If most people are working in clinics and we have some people working with a device firm or a start-up or a tech firm, is that good or bad? If we want the students to have enough in common across their experiences so that they can talk to each other and learn from each other, how will the difference in individual student experiences change the classroom experience? For instance, imagine that you are working with a start-up. They do not yet have operations on the ground in the host country. So what then do you do with the site visit? It is not at all like arriving at a clinic and walking through the waiting room with all the patients there. For a while I really tried to do only that clinical frontline, but every year I meet amazing entrepreneurs. Every year I put in at least one project that deals with something like a start-up in the device space. That’s definitely something I continue to revisit.